Other
Visual Summary – A review of nonsurgical neurolytic procedures for neuropathic pain
Nonsurgical physical and chemical neurolytic procedures may be used to treat neuropathic pain. Learn more.
Averitas Pharma

Disclaimer: The content presented may include information about products or uses that have not been approved by the US Food and Drug Administration. Averitas Pharma does not recommend the use of any products outside of their approved prescribing information. For full prescribing information, please refer to the approved product labeling. ---
Neuropathic pain can significantly impact quality of life and may not respond to conventional treatments such as oral medications, leaving over half of patients with inadequate pain reduction. As a result, symptoms often persist and become chronic.
Physical and chemical nonsurgical neurolytic procedures offer an option to alleviate neuropathic pain that does not respond to conventional treatments. These methods induce neurolysis by intentionally damaging peripheral nerves through freezing, heating, or application of chemicals, causing temporary degeneration of the affected nerve fibers and interrupting nerve signal transmission. Unlike central nervous system injury, peripheral nerves can regenerate following such damage.
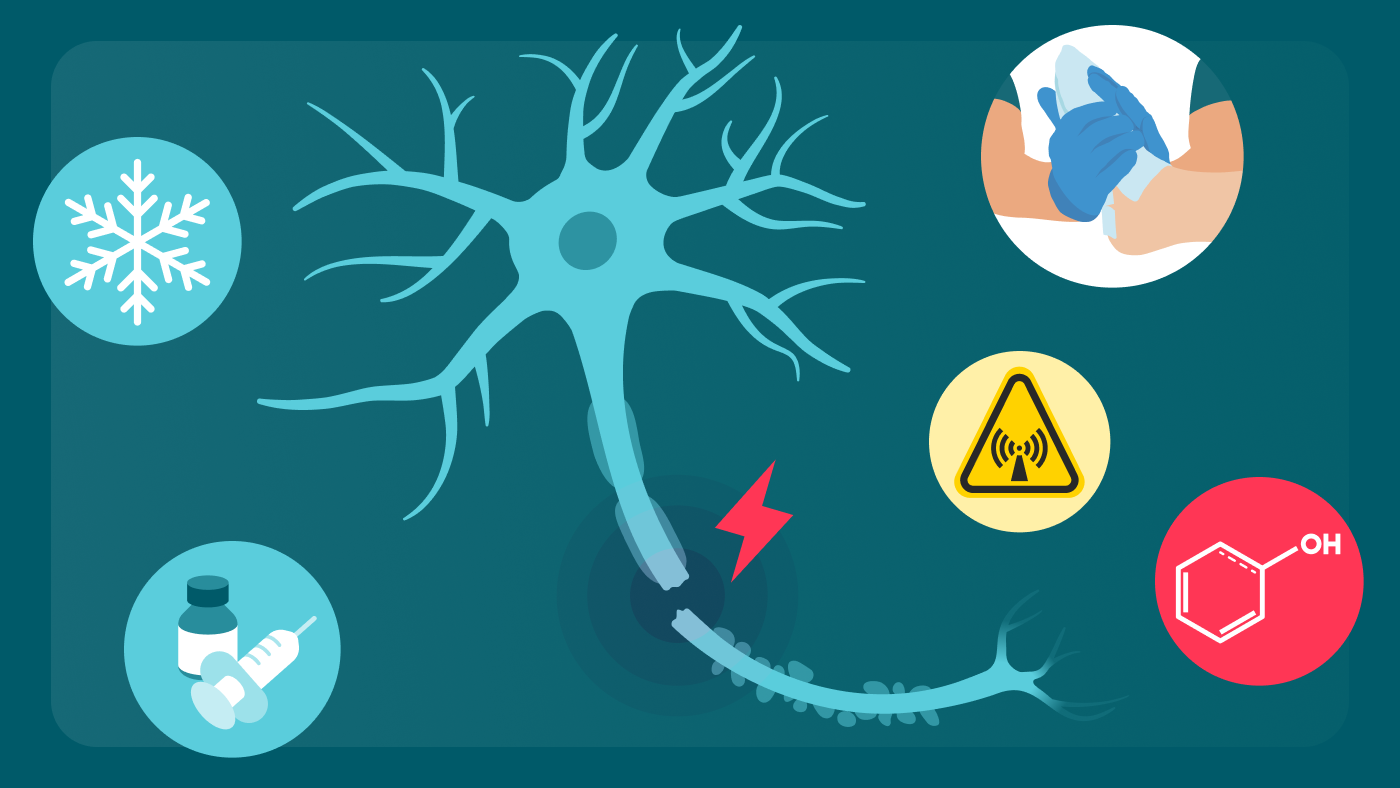
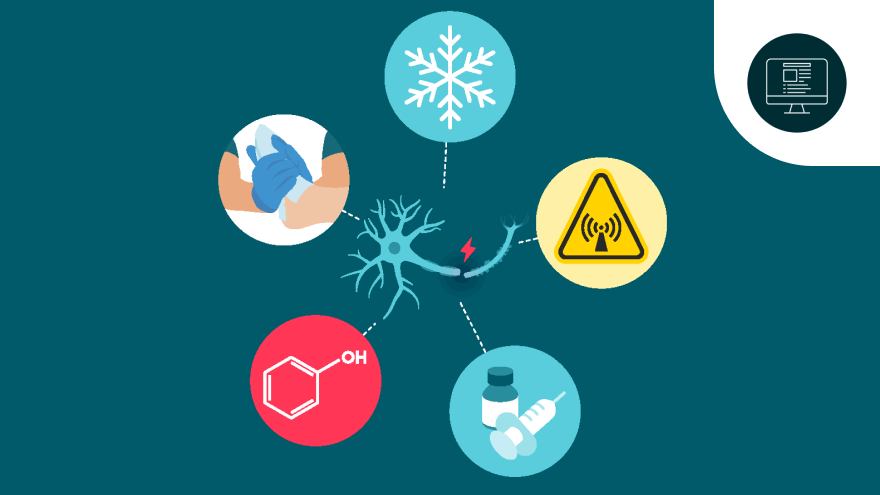
A narrative review by Gupta et al. provides a comprehensive overview of five nonsurgical neurolytic procedures commonly used to treat neuropathic pain and peripheral neuropathies. These include two physical procedures, cryoneurolysis and radiofrequency ablation, and three chemical procedures, namely alcohol or phenol injection and the capsaicin 8% topical system.
Limitations: In the review by Gupta et al., prospective analyses assessing the safety and efficacy of each neurolytic procedure were included where possible; however, for some procedures, available data were limited to case reports and anecdotal evidence. Additional limitations included reliance on a single database (PubMed), restriction to English-language publications, and potential bias inherent in the non-systematic methodology.
This narrative review considers the risk benefit basis of these nonsurgical neurolytic procedures and provides insight into their optimal utilization.
Cryoneurolysis utilizes extreme cold, whereas radiofrequency ablation employs heat to temporarily interrupt nerve conduction and relieve neuropathic pain. There is a risk of permanent nerve damage, which can be reduced by using ultrasound or fluoroscopy guidance during the procedures.
Alcohol or phenol injections function as nonselective chemoneurolytic agents causing degeneration of nerve fibers to provide pain relief. These treatments are typically considered therapies of last resort and are not approved in the USA for neuropathic pain. Ultrasound or fluoroscopy guidance is necessary for both procedures, and there is a risk of off-target tissue damage and post-treatment neuritis.
The capsaicin 8% topical system is approved in the USA for neuropathic pain associated with diabetic peripheral neuropathy of the feet. Capsaicin’s pain-modulating effects are driven by multiple mechanisms including selective binding to transient receptor potential vanilloid 1 (TRPV1) receptors on peripheral nociceptive fibers, reduced pain transmission to the brain, and temporary chemoneurolysis of TRPV1-expressing fibers. The most common adverse events are transient application-site reactions, such as burning, pain, and erythema.
Key takeaway: Nonsurgical neurolytic procedures offer an option for managing neuropathic pain but, as with any treatment, careful consideration of the risks and benefits is essential.
--- Footnote:
TRPV1, transient receptor potential vanilloid 1; USA, United States of America.
Gupta M et al. J Pain Res. 2025;18:879–95.
N/A-07-25-0011 | August 2025
Nonsurgical physical and chemical neurolytic procedures may be used to treat neuropathic pain. Learn more.
Discover more about the mechanism of action of the capsaicin 8% topical system

Information updated in August 2025.
INDICATION
In the USA, capsaicin 8% topical system is indicated for the treatment of neuropathic pain associated with postherpetic neuralgia (PHN) and neuropathic pain associated with diabetic peripheral neuropathy (DPN) of the feet.